Audit of the First Nations and Inuit Home and Community Care Program
September 2023
Prepared by: Audit and Assurance Services Branch
PDF Version (995 Kb, 23 pages)
Table of contents
Acronyms
| DCI |
Data Collection Instrument |
|---|---|
| e-HRTT |
Electronic Human Resources Tracking Template |
| e-SDRT |
Electronic Service Delivery Reporting Template |
| FNIHB |
First Nations and Inuit Health Branch |
| FNIHCC |
First Nations and Inuit Home and Community Care |
| FTE |
Full-Time Equivalents |
| HQ |
Headquarters |
| IBA |
Initial Budget Allocation |
| ISC |
Indigenous Services Canada |
| MOP |
Management Operational Plan |
| RO |
Regional Offices |
| SMC |
Senior Management Committee |
| TB |
Treasury Board of Canada |
Executive Summary
The First Nations and Inuit Home and Community Care (FNIHCC) Program provides funding and advice on developing home and community care services to Indigenous people living in First Nations and Inuit communities. The FNIHCC Program enables First Nations and Inuit individuals of all ages with disabilities, chronic or acute illnesses and the elderly to receive the care they need in their homes and communities. The First Nations and Inuit Health Branch (FNIHB) of Indigenous Services Canada (ISC) encompasses multiple programs, including the FNIHCC Program. FNIHB Headquarters (HQ) is responsible for overseeing the program and for providing funding for the FNIHCC Program. Program expenditures for fiscal year 2022-23 were approximately $170 million.
The objective of this audit was to provide assurance that the FNIHCC Program has implemented appropriate governance processes and collects relevant data to execute and inform program management and decision-making.
The audit concluded that the program has implemented key components of governance; however, opportunities for improvement were identified with respect to documenting funding decisions, reviewing and updating key program documentation as well as identifying their data needs.
At the time of this audit, the FNIHCC program was part of an engagement with Indigenous partners to identify opportunities for improving the program, including streamlining services and reimagining the delivery of these essential services to Indigenous communities. The findings from this engagement also highlighted opportunities for improvement related to the governance, challenges with funding of program services and data collection and utilization. The recommendations of this audit are not intended to override the outcomes of the engagement process but are meant to address identified issues in the interim.
The audit has resulted in the following recommendations:
- The Senior Assistant Deputy Minister of the First Nations and Inuit Health Branch, in collaboration with the Assistant Deputy Minister of Regional Operations of the First Nations and Inuit Health Branch, should ensure key program operational documents are reviewed, updated and approved at the appropriate level. Also, rationales for funding decisions should be documented and shared with regions for increased transparency.
- The Senior Assistant Deputy Minister of the First Nations and Inuit Health Branch, in collaboration with the Assistant Deputy Minister of Regional Operations of the First Nations and Inuit Health Branch, should ensure the data needs of the program are clearly identified and aligned with results and decision-making requirements prior to the implementation of recommendations for the ongoing Engagement for a Holistic Long Term and Continuing Care Framework. This will allow the program to participate more meaningfully when discussing the data requirements and approaches to obtaining the required data. Additionally, there should be an oversight mechanism to periodically validate data reliability and ensure measures to mitigate risk to data quality are working effectively with improvements being made as needed.
Statement of conformance
The audit conforms with the Institute of Internal Auditors' International Standards for the Professional Practice of Internal Auditing and the Government of Canada's Policy on Internal Audit, as supported by the results of the Quality Assurance and Improvement Program.
Management's Response
Management is in agreement with the findings, has accepted the recommendations included in the report, and has developed a management action plan to address them. The management action plan has been integrated into this report.
1. Context
The FNIHCC Program provides funding and advice on developing home and community care services to Indigenous people living in First Nations and Inuit communities. The FNIHCC Program enables First Nations and Inuit individuals of all ages with disabilities, chronic or acute illnesses and the elderly to receive the care they need in their homes and communities. The program strives to provide home and community care services for First Nations and Inuit equivalent to the services other Canadian residents receive.
The FNIHCC Program is delivered by home care registered nurses as well as trained and certified personal care workers. The FNIHCC Program has been authorized as a mandatory program and was co-developed with Assembly of First Nations and Inuit Tapiriit Kanatami in 1999.
Funding is provided on an annual basis through negotiated funding agreements to support service delivery to program recipients. The FNIHCC Program provides funding and has the authorityFootnote 1 for both essential home care servicesFootnote 2 and operation of services which support the delivery of the program. These services include:
- Client assessment;
- Case management;
- Home care nursing services;
- Home support and personal care;
- In-home respite;
- Palliative care;
- Linkages and referrals to other health and social services;
- Provision of and access to specialized medical equipment and supplies for care;
- Record keeping and data collection;
- Program management and supervision; and
- Training to deliver above-mentioned services
The FNIHCC Program also has the authority for supportive services such as meal programs, adult day care, wellness and fitness; however, these services are only funded if there are essential home care service funds remaining.
FNIHCC expenditures have increased since the program's inception. The increase in expenditures is a result of multiple factors including the addition of new communities to the program, expanding the services to include the palliative care resulting from Budget 2017 implementation, and additional COVID-19 related funding that was added to the contribution agreement portion of the FNIHCC program. This funding was used for the program response during the pandemic. Although COVID-19 started during FY2020-2021, additional funding related to COVID-19 was not provided by the program until FY2021-2022.
The following table outlines prior year expendituresFootnote 3.
| 2019-20 Expenditures | 2020-21 Expenditures | 2021-22 Expenditures | 2022-2023 Expenditures | |
|---|---|---|---|---|
| without COVID-19 funding | with COVID-19 funding | |||
| $148.3M | $155.6M | $191.2M | $257.9M | $169.8M |
Departmental Roles and Responsibilities
FNIHB funds and / or delivers multiple programs, including the FNIHCC Program. FNIHB HQ is responsible for facilitating research activities, maintaining working relationships with other federal departments, providing on-going communications and information to First Nations and Inuit on national developments that impact home and community care, facilitating the developmental and implementation activities of the program, national compilation of analysis and report preparation from a National perspective, and overseeing and ensuring completion of national evaluation and accountability activities. Regional offices (RO) are responsible for disseminating funding to recipients, for liaising with First Nations and Inuit stakeholders, and for providing oversight and monitoring on service delivery and data collection, amongst others.
Funding for this program is delivered through transfer payments and the Department's role is to manage the transfer payments to recipients. Recipients are responsible for delivering the program at the community level.
2. About the Audit
The Audit of FNIHCC Program was included in the Indigenous Services Canada 2022-2023 to 2023-2024 Risk-Based Audit Plan, which was presented to the Audit Committee and approved by the Deputy Minister in June 2022.
2.1 Why is it Important
The audit was identified as a priority because the Department has identified several risks for health services, and as such, it is important to ensure that the program has effective governance mechanisms and the right data to make key decisions related to the delivery of funding and services for program recipients.
2.2 Audit Objective
The audit objective was to provide assurance that the FNIHCC Program has implemented appropriate governance processes and collects relevant data to execute and inform program management and decision-making.
2.3 Audit Scope
The scope of the audit included the FNIHCC Program's processes and activities, both at HQ and in the regions, that support the delivery of the program.
To cover program processes and activities in place both pre-COVID-19 and during COVID-19, the audit covered the period from April 1, 2018, to September 30, 2022.
The audit examined four Indigenous Services Canada (ISC) regional offices, which were selected based on the following criteria:
- Funding allocations and expenditures;
- Recipient funding agreement types (set, fixed, flexible, and block funding approaches; and the New Fiscal Relationship (NFR) 10-year Grant)); and
- Program recipients types (First Nations and Inuit)Footnote 4.
The regions selected for inclusion in the scope of the conduct phase were Ontario, Manitoba, Saskatchewan, and the Northern Region. The Northern Region includes the Northwest Territories, Nunavut, and Yukon. However, Yukon was scoped out because 94.4% of the funding provided to the Northern Regions goes to the Northwest Territories and NunavutFootnote 5. These four regions represent 67% of the total Vote 10 FNIHCC expenditures and 75% of the total NFR Grant (Vote 10) FNIHCC expenditures for the fiscal years 2020-2021, 2021-2022, and 2022-2023.
The audit did not cover processes and activities in place within funding recipient organizations. The audit also did not include engagement activities as they were ongoing at the start of the audit and initial regional results of the engagement activities had not been finalized.
2.4 Audit Approach and Methodology
The audit was conducted in accordance with the requirements of the Treasury Board of Canada (TB) Policy on Internal Audit and was conducted in accordance with the Institute of Internal Auditors' International Standards for the Professional Practice of Internal Auditing. The audit examined sufficient, relevant evidence and obtain sufficient information to provide a reasonable level of assurance in support of the audit conclusion.
The audit was performed from August 2022 to September 2023 and consisted of three phases: planning, conduct and reporting. The main audit methods used included:
- Interviews with key stakeholders involved in the governance processes and the collection of data;
- Process walkthroughs with HQ and each in-scope regions to assess governance structures, accountability frameworks, decision-making processes, and roles and responsibilities within the FNIHCC program;
- Documentation review including procedures in place to review governance, to ensure governance is effectively carried out within the program, and documentation related to obtaining and communicating the feedback and input from First Nations and Inuit Stakeholders; and
- Documentation review including examining the sources of data, the guidance outlining the data required for decision making, and the guidance used to validate reliability of data.
The approach used to address the audit objective included the development of audit criteria, against which observations and conclusions were drawn. The audit criteria can be found in Annex A.
3. Key Findings and Recommendations
3.1 Governance
Background
Governances refers to the structures, systems, and practices in place to:
- Assign decision-making authorities, define the decision-making process, and establish the organization's strategic direction;
- Oversee the delivery of its services, the implementation of its policies, plans, programs, and projects;
- Monitor and mitigate key risks; and
- Report on its performance in achieving intended results and using performance information to drive ongoing improvements and corrective actions.Footnote 6
Governance practices are important to ensure that the program is performing effectively against its objectives and that the program is sufficiently funded to effectively deliver its essential home care services within communities and maintain substantive equality with home and community care services provided to other Canadian residents.
Given the importance of governance within an organization, the audit expected there to be governance structures, systems, and practices, including:
- Program governance structures to set direction and clearly assign program roles, responsibilities, and decision-making authorities;
- Governance mechanisms to ensure that program roles, responsibilities, oversight, and decision making are carried out as intended; and
- Processes to obtain and integrate relevant stakeholder input with program delivery.
There was a risk that governance of the FNIHCC Program is not properly designed, implemented and effectively carried out. This may result in the FNIHCC Program not meeting its objectives and not being delivered with appropriate stakeholder representation.
Finding
Governance Structures
The audit reviewed program governance structures that set direction and clearly assign program roles, responsibilities, and decision-making authorities. As such, governance structures (i.e. roles and responsibilities, and decision-making authorities) should be defined, documented and established in alignment with the objectives of both the program and the Department. Establishing these structures would allow the program to effectively deliver home and community care services, assess program performance and make program specific decisions. Regularly reviewing these structures would ensure continued alignment with program and departmental objectives in an evolving health environment.
The audit found that there are defined roles and responsibilities related to program management and decision-making for both HQ and at the regional level (i.e., FNIHB and FNIHB-RO) which were found in the FNIHCC Program Description and Implementation Plan (1999). The audit also found that there is a draft FNIHB Accountability Framework (2022), which defines the decision-making authorities and interactions among the various branch directorates and between the national and regional offices, while aligning with broader departmental strategic objectives, as well as the health and wellbeing of First Nations and Inuit. At the time of the audit, the FNIHB Accountability Framework (2022), although never formally approved and remained labelled as draft, was shared, and used by the program.
The program governance starts with the Senior Management Committee (SMC) at FNIHB. The FNIHB SMC Terms of Reference outlines the membership which includes amongst others the Assembly of First Nations, Inuit Tapiriit Kanatami, FNIHB Senior Assistant Deputy Minister, FNIHB RO Assistant Deputy Minister, Director General Primary Health Care, and Regional Executives. There is also the FNIHCC Regional Coordinators Working Group, which provides regional and national updates on the FNIHCC Program.
Although there is documentation that defines the governance structures as well as roles and responsibilities in the program, the audit found that this documentation is not periodically reviewed for relevance and completeness. For example, there are instances of program documentation that has not been updated since the program was created in 1999, such as the FNIHCC Program Description and Implementation Plan as well as the Program Framework. There are also branch-wide documents that are used at the program level that have remained in draft and not formally approved, such as the FNIHB Accountability Framework (2022). There were also inconsistencies noted among regions on whether roles and responsibilities have been updated. These inconsistencies are due to draft and outdated documentation since program implementation. It was noted during the audit that outdated documentation was more prominent when FNIHB was consolidated with ISC and the program has been unable to update their documentation due to the additional backlog the consolidation created. Periodic reviews on the established governance structures and documentation related to program governance may provide an opportunity for the program to re-assess whether roles and responsibilities have evolved. As such, having documented guidance or procedures to regularly review, update and approve program and governance documentation would ensure this is done consistently.
While the audit noted the existence of some governance structures within the FNIHCC Program, the following subsections outline the gaps that were identified in the implementation of governance.
Funding Approval
Additionally, the audit reviewed decision-making processes in relation to funding, which is a governance mechanism that falls under the program's responsibilities. The FNIHCC Program receives ongoing funding, with an annual growth applied. The funds are ultimately distributed to the communities through the regions based on a funding formula established in 1999. The funding formula was co-developed with partners and was required to be based on the national essential services elements of the program, to support current service delivery patterns and the variety of federal funding agreements and respect the Assembly of First Nations Annual General Assembly Chief's resolution. The funding formula is comprised of four components: service delivery, program management, operating, and community remoteness.
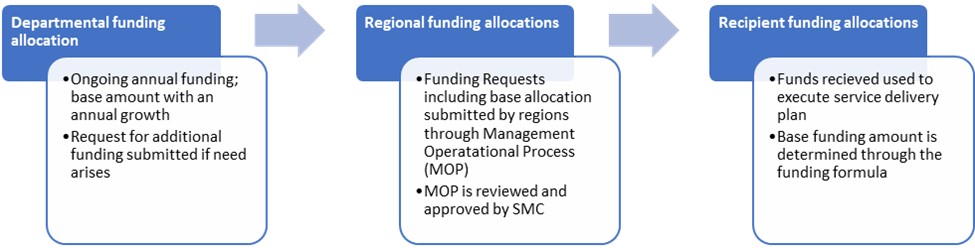
Text alternative for Figure 1 – Funding Allocation Steps
Figure 1 provides an overview of the departmental funding allocation process for the FNIHCC Program.
The steps illustrated in the departmental funding allocation process for the FNIHCC Program (figure 1) are as follows:
- Departmental Funding Allocation
- Ongoing annual funding; base amount with an annual growth
- Request for additional funding submitted if need arises
- Regional Funding Allocations
- Funding Requests including base allocation submitted by regions through the Management Operational Process (MOP)
- MOP is reviewed and approved by the Senior Management Committee (SMC)
- Recipient Funding Allocations
- Funds received used to execute service delivery plan
- Base funding amount is determined through the funding formula
As outlined in Figure 1, through a departmental process, the program currently receives their Initial Budget Allocation (IBA) with a growth escalator applied annually. The IBA amount for the program was initiated in 1999, with small increases for training and wage parity in the early 2000's. Growth was included in mid to late 2000's and has been ongoing, as per the regional decision-making process. Budget 2017, which provided the program with funding increases over a five-year period, has been deemed ongoing and is added to the program's base amount going forward.
The total funds received by the Department annually are allocated to each region, then distributed to the recipients. This process is managed at HQ with regional input and approved by appropriate authorities in FNHIB. Regions can also request additional funds to meet funding pressures or community requests through the Management Operational Plan (MOP) process at the beginning of each year. Annually, each funding recipient receives their base funding amount with an annual growth. This base amount was calculated at inception of the program or when the community joined the program and is not updated to reflect any changes to the components of the formula.
The audit observed that the approval for base funding and additional funding requests are determined by ISC's SMC. Their decision is documented in the MOP along with the date of SMC's decision. For approval of funding and funding requests, there is no further information provided other than approval and date of approval of funding requests within the MOP. However, it was observed that in instances where funding was rejected, no justification to support the final decision was documented in the MOP. In addition, these justifications related to the rejection of funding requests were not communicated with the regions or the communities that requested the funding.
A review of the MOPs provided for the period of the audit shows that funding request denials were related to additional funding pressures put forward by the regions. Some of the instances identified were for funding services that the program currently has the authority for, but not the funding to deliver, such as footcare services. However, the audit also noted instances where a request was on the MOP to obtain and provide funding to deliver the program to new communities, to provide training and certification to health care providers. The audit observed these instances of funding not approved, and in these instances, a rationale was not provided. The tables below demonstrate the additional funding pressures requested within the FNIHCC Program for fiscal year 2018-2019 to 2022-2023 and the total amount requested for all regions and for in-scope regions.
| MOP | Additional Funding Pressure Requested | Additional Funding Pressure Not Provided | Total Amount Requested | Total Amount Provided |
|---|---|---|---|---|
| 2018-2019 | 9 | 8 | $1,021,128.00 | $89,000.00 |
| 2019-2020 | 15 | 12 | $2,548,992.00 | $984,642.00 |
| 2020-2021 | 2 | 0 | $230,281.00 | $230,281.00 |
| 2021-2022 | 1 | 1 | $1,000,000.00 | $0.00 |
| 2022-2023 | 11 | 11 | $5,094,667.00 | $0.00 |
| MOP | Additional Funding Pressure Requested | Additional Funding Pressure Not Provided | Total Amount Requested | Total Amount Provided |
|---|---|---|---|---|
| 2018-2019 | 3 | 2 | $ 465,000.00 | $0.00 |
| 2019-2020 | 2 | 1 | $612,500.00 | $0.00 |
| 2020-2021 | 1 | 0 | $198,281.00 | $198,281.00 |
| 2021-2022 | 1 | 1 | $1,000,000.00 | $0.00 |
| 2022-2023 | 6 | 6 | $3,460,026.00 | $0.00 |
For those additional funding requests that are denied without a properly documented and sound rationale, the program cannot be certain that clear actions are taken arising from these decisions, and appropriate accountabilities are made to support the continuous improvement of the FNIHCC Program. This could also impact the ability of the program to provide high quality health services and respond to and support the needs of the communities.
Integration of Stakeholder Input
The audit reviewed processes to obtain and integrate relevant stakeholder input with program delivery. The audit found that there are documented processes at the regions to obtain feedback from First Nations and Inuit Stakeholders. Regions have adopted consistent practices to obtain feedback based on their individual relationships with the communities.
The audit examined how the feedback and input received by the regions is integrated into the program. It was noted by the regions that most of the feedback obtained is related to identifying funding or service needs. Several examples were observed in the regions such as palliative care funding, new community funding, footcare services funding, improved healthcare record systems, and the need for funding of in-home dialysis services. Regions would communicate these community identified needs to HQ through funding requests on the MOP, or to national working groups through other means. However, as mentioned in the previous section, not all the requests for additional funds are approved or available to provide to the communities.
The audit noted that there used to be a national network that involved First Nations and Inuit partners from across all regions, used as a key communication structure that was dismantled in 2016. Although the audit could not determine why the network was dismantled, the program stated that there have been recent conversations to reinstate this network streamline and improve the communication process.
Overall, the audit noted governance structures are defined and communicated; however, processes to review, update, and approve key program documents, including governance information, are currently not in place. While oversight mechanisms and decision-making authorities related to funding are implemented and defined, consideration should be made on documenting the rationale for funding decisions for improved transparency and to identify potential opportunities for improvement. This may impact the delivery and operations of the FNIHCC Program, which may lead to a substantial loss of stakeholder confidence.
At the time of this audit, the FNIHCC program was part of an engagement with Indigenous partners to identify opportunities for improving the program, including streamlining services and reimagining the delivery of these essential services to Indigenous communities. The findings from this engagement also highlighted opportunities for improvement related to the governance and funding of program services. The recommendations of this audit are not intended to override the outcomes of the engagement process but are meant to address identified weaknesses in the interim.
Recommendation
The Senior Assistant Deputy Minister of the First Nations and Inuit Health Branch in collaboration with the Assistant Deputy Minister of Regional Operations of the First Nations and Inuit Health Branch should ensure key program operational documents are reviewed, updated and approved at the appropriate level. Also, rationales for funding decisions should be documented and shared with regions for increased transparency.
3.2 Data to Support the FNIHCC Program
Background
Data collection to carry out program monitoring, ongoing planning, reporting, and evaluation activities is listed as one of the nine essential services of the FNIHCC Program. Agreements with FNIHCC recipients required the submission of data and financial reports to fulfill the mandatory program reporting requirements and to demonstrate appropriate usage of funds.
The audit expected the Program to have an effective data collection approach to help ensure that program officials can access and leverage relevant and reliable data to inform program related decisions, such as funding and service delivery decisions.
Specifically, the audit expected to see the following related to the data currently being collected:
- Data collected is relevant and supports the program in identifying and tracking the needs of the communities, supports the program in its decision-making including program funding, and the overall delivery of the program; and
- Sufficient processes to help minimize errors in manually entered data at the community level.
There was a risk that relevant and reliable data is not being collected and used by the program, and that the program has not defined its data needs, therefore impacting program management and the decision-making process.
Finding
Relevant Data
Ensuring the program has relevant, complete and accurate data available is essential so that informed decisions can be made to achieve the desired objectives of the program. Additionally, the collection of relevant data allows the program to identify areas of improvement and ultimately better understand the needs of recipients.
The main sources of data reporting for the FNIHCC Program that were examined during the audit were through the Electronic Service Delivery Reporting Template (e-SDRT), Electronic Human Resources Tracking Template (e-HRTT), and the FNIHCC Program Data Collection Instrument (DCI). Data currently collected through the e-SDRT and e-HRTT is used to support the overall program through areas such as resource allocation, training, and identifying health trends within recipient communities. The program has stated their objective to transition to the DCI as the primary source of data collection. Table 4 below highlights the three main data sources and the related data they collect:
| Data Source | Data Collected | Frequency of Report Submission |
|---|---|---|
| e-HRTT | Tracks the types of employees First Nations and Inuit Communities have on staff, their education and working hours | AnnuallyFootnote 7 |
| e-SDRT | Tracks the type and quantity of services the client has received along with client demographics | Annually |
| FNIHCC Program DCI | Summary of the data found both in e-HRTT and e-SDRT. The DCI is broken up into four categories:
|
Annually |
The audit found that, amongst other things, regions can utilize the data collected to assess individual communities' specific health needs and trends by reviewing data related to the services provided (collected in e-SDRT) against the number of full-time equivalents (FTEs) staffed by the community (collected in e-HRTT). By comparing key data points, regions are able to have conversations with communities to help identify needs on the ground.
Moreover, the audit found that regional decisions are driven by the data collected and the program uses the data collected to meet its reporting requirements. However, the most notable area of how data collected could potentially be used was related to the funding of the program. The program is funded through an allocation-based model, and recipient allocations were based on the funding formula that was co-developed with Partners in 1999 when the program was launched. The base-allocation which was determined through inputting projected population figures from 1997, is out of date and has not been revised since its creation, even though the FNIHCC Program has access to more accurate data that could be inputted into the funding formula (recent census figures, etc.). While this may be a result of an outdated funding formula, the program is currently working on an analysis of the demand and cost forecasts for the program. However, if the current funding approach were to change, potentially requiring data to support funding decisions, the program currently has not identified its data needs required to support potential changes or have all the data to support a robust funding analysis.
Transition to the FNIHCC DCI
The FNIHCC DCI template was introduced departmentally to reduce the reporting burden on recipients. Currently the DCI provide high level data points related to FTE and client counts. The e-SDRT and e-HRTT provides more details related to health services provided and Individual demographic information.
Table 5 below highlights an example of data from e-SDRT and e-HRTT and data from the FNIHCC DCI.
| Data Presented in e-SDRT and e-HRTT | Summarized Data Field in DCI |
|---|---|
| Primary Reason For Care Frequency of Services Provided Hours of Service Provided |
Number of Home Care Clients Accessing Home Care Services |
As evident from the table above, while the DCI provides information related to the number of clients benefitting from the program, it does not provide the specific data related to the service provided and its frequency, which could be used by the program to allocate its resources to support community needs. Given the program's intention to shift to the DCI as the primary source of data, it is important that the DCI template is assessed to validate that all relevant data currently captured in the e-SDRT and e-HRTT are not omitted. While this has been acknowledged by the FNIHCC Program, there has been no formalized plan to assess the DCI template.
The data currently collected by the program remain relevant in identifying health trends in recipient communities. However, it was observed that the program does not have processes in place to identify their data needs related to funding or processes to periodically review their data sources. These observed gaps are likely due to the result of an absent data strategy, which could result in misinformed program funding decisions that do not support the evolving health needs.
Reliability of Data Collected
Data collected by the FNIHCC Program present a risk as they are self-reported and are entered at the user level. However, it was observed that the program has mechanisms in place at the regional level to help prevent potential data quality issues. These mechanisms include:
- providing training to users;
- conducting check-ins with communities to verify any data outliers; and
- providing clear instructions for the completion of data templates.
However, there is no oversight mechanisms in place at the HQ level to ensure that the regions are implementing mechanisms mentioned to help addressing potential data reliability issues. This may because the data collected by the program is not used to support key decisions at a national level such as funding. Additionally, the FNIHCC DCI has noted gaps, which may result in relevant information no longer being captured. These shortcomings could potentially result in misinformed program decision making.
As previously mentioned, the FNIHCC program was part of an engagement with Indigenous partners to identify opportunities for improving the program at the time of this audit. The findings from this engagement also highlighted opportunities for improvement related to how data is collected and utilized. As previously mentioned, recommendations of this audit are not intended to override the outcomes of the engagement process but are meant to address identified weaknesses in the interim.
Recommendation
The Senior Assistant Deputy Minister of the First Nations and Inuit Health Branch, in collaboration with the Assistant Deputy Minister of Regional Operations of the First Nations and Inuit Health Branch, should ensure the data needs of the program are clearly identified and aligned with results and decision making requirements prior to the implementation of recommendations for the ongoing Engagement for a Holistic Long Term and Continuing Care Framework. This will allow the program to participate more meaningfully when discussing the data requirements and approaches to obtaining the required data. Additionally, there should be an oversight mechanism to periodically validate data reliability and ensure measures to mitigate risk to data quality are working effectively with improvements being made as needed.
4. Conclusion
The audit concluded that, overall, the program has implemented some key components of governance, including defined roles, responsibilities, and decision-making authorities. However, opportunities for improvement were identified, including implementing timely reviews and updates of governance frameworks and key program documentation, as well as improving documented decisions, specifically related to program funding requests that arise from stakeholder feedback. There is a risk that these identified gaps could potentially result in the program not meeting its objectives as health needs of communities evolve. There is also an opportunity for the program to clearly identify their data needs and ensure those data requirements are aligned with key results and decision making needs of the sector.
5. Management action plan
In the course of performing separate audits of the Assisted Living Program and the First Nations and Inuit Home and Community Care Program, it was identified that both programs are linked with the broader Long Term and Continuing Care (LTCC) engagement and framework development. Despite the distinct nature of each audit, the recommendations derived were found to be mutually relevant, primarily because they align with the overarching findings and objectives of the LTCC engagement. Consequently, a shared management action plan has been adopted for both programs. This approach ensures a cohesive and efficient response to the recommendations, fostering the co-development of policy options within a distinctions-based LTCC framework. Therefore, readers will notice recommendations from one program's audit reflected in the management action plan of the other, and vice versa, emphasizing a unified strategy to enhance LTCC-related services.
| Recommendations | Management Response / Actions | Responsible Manager (Title) | Planned Implementation Date |
|---|---|---|---|
| Assisted Living Program Audit Recommendation #1: The Assistant Deputy Minister of Education and Social Development Programs and Partnerships (ESDPP), in consultation with relevant stakeholders, should leverage the ongoing Engagement for a Holistic Continuum of Long Term and Continuing Care to improve the alignment of the Assisted Living Program funding approach with client needs. Implementing this new approach should involve identifying relevant data sets, both currently available and any new data requirements, to improve the forecasting and predictive capabilities of the model. First Nations and Inuit Home and Community Care Audit Recommendation #2: The Senior Assistant Deputy Minister of the First Nations and Inuit Health Branch (FNIHB), in collaboration with the Assistant Deputy Minister of Regional Operations of the First Nations and Inuit Health Branch (FNIHB-RO), should ensure the data needs of the program are clearly identified and aligned with results and decision making requirements prior to the implementation of recommendations for the ongoing Engagement for a Holistic Continuum of Long Term and Continuing Care. This will allow the program to participate more meaningfully when discussing the data requirements and approaches to obtaining the required data. Additionally, there should be an oversight mechanisms to periodically validate data reliability and ensure measures to mitigate risk to data quality are working effectively with improvements being made as needed. |
The Assistant Deputy Minister of Education and Social Development Programs and Partnerships (ESDPP), along with the Senior Assistant Deputy Minister and the Assistant Deputy Minister of the First Nations and Inuit Health Branch (FNIHB) agree with this recommendation. Long Term and Continuing Care (LTCC) engagement activities with First Nations and Inuit partners concluded in Fall 2022 and the co-development of policy options on a distinctions-based LTCC framework started in Spring 2023 with results to be presented in Winter 2024. It is expected that new data requirements will be required to address the resulting LTCC framework. ISC is committed to co-developing the implementation of the LTCC framework with First Nation and Inuit partners. To address this recommendation specifically, ESDPP and FNIHB will:
|
ADM, ESDPP SADM, FNIHB ADM, FNIHB-RO |
June 2024 – Research on existing data in preparation for First Nations and Inuit partners discussions August 2025 – finalized data requirements. Full implementation March 31, 2026 |
| Assisted Living Program Audit Recommendation #2: The Assistant Deputy Minister of Education and Social Development Programs and Partnerships (ESDPP), in collaboration with the Senior Assistant Deputy Minister of Regional Operations and the Associate Assistant Deputy Minister of Regional Operations, should establish a framework that includes clearly defined outreach roles and responsibilities and associated guidance to help ensure that outreach activities are carried out effectively and that material disseminated to First Nation communities is accessible, complete, and accurate to ensure all those that need the services of the program are aware and able to access it. |
The Assistant Deputy Minister of Education and Social Development Programs and Partnerships, and the Senior Assistant Deputy Minister of Regional Operations agree with this recommendation. It is anticipated that the new outreach framework will clarify roles and responsibilities including timeframes and methods for disseminating changes to First Nation partners. ESDPP will work with colleagues from the Regional Operations Sector to develop the new outreach framework document to provide consistency and clarity to First Nations. The new outreach framework document will be reviewed yearly with regions to ensure it is kept up to date. Note: ESDPP will also collaborate with FNIHB HCC on communication roles and responsibilities and will align messaging to First Nations as appropriate. |
ADM, ESDPP SADM, RO |
March 31, 2024 |
| First Nations and Inuit Home and Community Care Program Audit Recommendation #1: The Senior Assistant Deputy Minister of the First Nations and Inuit Health Branch, in collaboration with the Assistant Deputy Minister of Regional Operations of the First Nations and Inuit Health Branch, should ensure key program operational documents are reviewed, updated and approved at the appropriate level. Also, rationales for funding decisions should be documented and potentially shared with regions for increased transparency. |
The Senior Assistant Deputy Minister and the Assistant Deputy Minister of the First Nations and Inuit Health Branch (FNIHB) agree with this recommendation. In alignment with this recommendation:
|
SADM, FNIHB ADM, FNIHB-RO |
Documentation of funding decisions rationales – April 2024 Updated Key operational documents - March 31, 2025 and ongoing |
Annex A: Audit Criteria
To ensure an appropriate level of assurance to meet the audit objectives, the following audit criteria were developed to address the objectives.
Audit Criteria
- FNIHCC Program governance has been implemented for overseeing program management and supporting decision making.
- Governance structures, accountability frameworks and roles and responsibilities have been defined and are communicated to FNIHCC Program employees and are effectively carried out.
- Processes for obtaining First Nations and Inuit stakeholder input relevant to the program are in place.
- Program management, delivery and decision making are informed by First Nations and Inuit stakeholders' input
- Data collected by the program is relevant and reliable and is used to inform program management and decision making.
- Data collected by the program is relevant and reliable to program management, supports program decisions, and improves accountability and delivery of the program.
- Analysis is performed by the program to rationalize that the data collected is relevant and reliable to achieving program objectives.
- Input is sought and gathered from representatives of First Nations and Inuit stakeholders to determine relevance of data collected.