Evaluation of the Aboriginal Health Human Resources Initiative 2013-2014 to 2017-2018
September 2019
Evaluation and Policies Re-Design Branch
Strategic Policy and Partnerships Sector
PDF Version (506 Kb, 33 Pages)
Table of contents
List ofAcronyms
| AFN |
Assembly of First Nations |
|---|---|
| AHHRI |
Aboriginal Health Human Resource Initiative |
| ESDPP |
Education and Social Development Programs and Partnerships |
| FNIHB |
First Nations and Inuit Health Branch |
| HHR |
Health Human Resource |
| ISC |
Indigenous Services Canada |
| ITK |
Inuit Tapiriit Kanatami |
Summary
This evaluation of the Aboriginal Health Human Resources (AHHRI) Initiative was conducted in compliance with the Treasury Board Policy on Results and the Financial Administration Act. The purpose of the evaluation was to provide a neutral and evidence-based assessment of the relevance and performance of the program, and to inform decision making related to program design and implementation as well as possible future directions. Due to the size of the AHHRI, the evaluation used a calibrated approach that focused on the use of qualitative data and existing monitoring data.
Aboriginal Health Human Resources Initiative
Project Profile
Through contribution agreements, the AHHRI aims to increase the number of First Nations, Inuit and Métis workers in the health care field, and to ensure that community-based workers are trained and certified to improve the quality and consistency of health care services provided in First Nations and Inuit communities.
Prior to December 2017, the AHHRI was delivered by Health Canada through the First Nations and Inuit Heath Branch (FNIHB). In December 2017, FNIHB was transferred to Indigenous Services Canada. Despite this change in departments, FNIHB continues to deliver the AHHRI.
Evaluation Scope and Methodology
The evaluation was completed in 2018-19 by Health Canada's Office of Audit and Evaluation and approved by Indigenous Services Canada (ISC).
The AHHRI provides funding through two streams. The evaluation examined the relevance, performance and efficiency of AHHRI Streams 1 and 2 from 2013-14 to 2017-18. Specifically, all Stream 1 activities delivered across Canada and Stream 2 activities delivered in every FNIHB region except British Columbia were examined. In British Columbia, responsibilities for federal health programs for First Nations have been transferred to the First Nations Health Authority in 2011.
Program Resources
- Stream 1 - ($3.0 million/year) – provides funding to Indspire, an Indigenous-led registered national charity, for scholarships and bursaries to First Nations, Inuit and Metis students in post‑secondary education programs that lead to health careers.
- Stream 2 ($1.5 million/year) – provides funding for the training of community based health care workers and health managers (in non-registered professions) working in health promotion and disease prevention in First Nations and Inuit communities.
The results of this evaluation are based on information collected through:
- Document and literature review;
- A review of Indspire annual monitoring reports and surveys of recipients; and,
- Interviews with 31 key informants from FNIHB national and regional program staff, associations of Indigenous health professionals; national Indigenous organizations; university student support services; and regional and community-based Indigenous health services organizations.
Key Findings
Relevance
There is a continued need to increase the number of Indigenous health workers, address financial barriers to accessing health studies and continue developing the capacity of First Nations and Inuit community health workers.
AHHRI's objectives align with Indigenous priorities around increasing the ability of communities to control their health services; increasing the number of Indigenous health workers and increasing the capacity of health workers in Indigenous communities. As well, the Government of Canada has consistently reiterated similar priorities over the last couple of years.
There exists a variety of other programs similar to AHHRI but there is no clear evidence of duplication as those other programs target very specific groups or geographic locations.
Performance – Stream 1
- Through Indspire, a total of 3,064 scholarships and bursaries were awarded over the evaluation period; helping approximately 765 Indigenous students per year to participate in health post‑secondary studies.
- The financial assistance covered approximately 17 percent of student's financial needs and is perceived helping to pursue their education. It is not known if students would have been able to access their health studies without AHHRI's funding.
- The majority of students helped through AHHRI Stream 1 worked in a field related to their studies and served Indigenous population as part of their work.
- The Indspire application process for financial assistance is seen as being difficult for students to complete, especially for the level of funding provided.
- Prospective students often don't have the prerequisite education to access health studies and there is a need to do more to prepare them for post-secondary health studies.
Overall, AHHRI is more focused on helping students to complete their studies as opposed to increasing the number of Indigenous students in health studies.
Performance – Stream 2
- AHHRI Stream 2 funding is seen as helping to increase the qualifications of health workers in communities as well as contributing to improve health services.
- AHHRI has contributed to improving the capacity of First Nations communities to influence and control their health services by funding the creation of the First Nations Health Managers Association and the establishment of its certification program for health managers. This certification program is seen as improving the management capacity within communities.
- Challenges related to the design and delivery of Stream 2 pertain to the limited amount of funding compared to the existing needs, and the types of training that are eligible for funding.
Efficiency
Approximately 80 percent of the contribution provided to Indspire was redistributed to students. Considering that Indspire is actively engaged in outreach activities and promoting studies, the delivery of Stream 1 activities by this organisation allows some leveraging of resources, which can contribute to achieving AHHRI objectives.
Practices have been put in place in FNIHB regions to coordinate decision making around allocation of funding with First National and Inuit organisations or provinces and territories. However, planning could be improved to meet community health resources needs.
Recommendations
The findings from this evaluation have led to the following two recommendations:
Recommendation 1:
ISC should work with Indspire to increase accessibility to post‑secondary education in the health field by:
- Streamlining the application process to make it easier to complete;
- Developing supports to help students complete prerequisite courses; and
- Building on existing outreach activities to increase the promotion of health careers across communities.
Recommendation 2:
ISC should ensure that training activities meet the needs of communities by:
- Engaging with communities to determine the best way to utilise the Stream 2 funding; and
- Increasing the coordination of AHHRI training activities with other similar ISC initiatives.
Management Response / Action Plan
Project Title: Evaluation of the Aboriginal Health Human Resources Initiative 2013-2014 to 2017-2018 This Management Response and Action Plan has been developed to address recommendations resulting from the Evaluation of the Aboriginal Health Human Resources Initiative (AHHRI), which was prepared by the Health Canada, Office of Audit and Evaluation and finalized by the Evaluation, Performance Measurement and Review Branch. The First Nations and Inuit Health Branch recognizes the findings highlighted by the Evaluation regarding the relevance and performance of the program. Specifically: The evaluation provides two recommendations to improve the design and delivery of the program. All recommendations are accepted by the program and the attached Action Plan identifies specific activities to move towards meeting these recommendations. It is important to note for Recommendation #1: A and C, the application process and outreach activities are beyond the scope of the Department as funding for the application process and outreach activities are developed and delivered by a non-governmental organization (Indspire). The Department will engage in talks with Indspire and make every effort to encourage them to take action in these items. The AHHRI has a limited program scope and associated budget ($4.5 million annually for both streams) with no additional source of funding to address any issues outside of the program's scope. The Department will leverage other work underway within the Department, including that of the Education and Social Development Programs and Partnerships (ESDPP) on advancing Indigenous Post-Secondary Education. 1. ISC should work with Indspire to increase the accessibility to post secondary education in the health field by: We agree with this recommendation and will engage in talks with Indspire regarding recommendations A and C in order to streamline the application process for students and increase the promotion of health careers. Recommendation B will be addressed by the ISC - ESDPP’s University and College Entrance Preparation Program, which provides financial assistance to First Nation and eligible Inuit students enrolled in university or college entrance programs to help them obtain the academic level required to enter a degree and anticipated funding included in the proposed Inuit and Métis Nation strategies. Action Items: 2. ISC should ensure that training activities meet the needs of communities by: We agree with this recommendation and will engage with regional partners/communities and initiate a call out ensuring a training plan has been developed. We will also work to increase the coordination of and communication about AHHRI training activities with other program areas by sending out the AHHRI training guidelines to program areas. Once the Management Operational Plan has been approved, the approved list of activities will also be sent out. Action Items:
1. Management Response
2. Action Plan
Recommendations
Actions
Responsible Manager (Title / Sector)
Planned Start and Completion Dates
Actions We ___DO__ concur.
(do, do not, partially)Manager, Quality Improvement and Accreditation Program
Start Date: April 2019
Completion:
March 2020
Actions We ___DO__ concur.
(do, do not, partially)Improvement and Accreditation Program
Start Date: April 2019
Completion: March 2020
Introduction
1.1 Evaluation Purpose
The Aboriginal Health Human Resources Initiative (AHHRI) was evaluated to assess the relevance, performance, and efficiency of the program for the period of April 2013 to March 2018. This program is delivered by the First Nations and Inuit Health Branch (FNIHB) of Indigenous Services Canada (ISC). Prior to December 2017, the FNIHB was located within Health Canada and the program was delivered under the auspices of Health Canada. The evaluation was initiated and conducted by the Office of Audit and Evaluation of Health Canada and subsequently submitted to Indigenous Services Canada for approval.
The evaluation was required in accordance with Section 42.1 of the Financial Administration Act, which stipulates that departments conduct a review of the relevance and effectiveness of ongoing program of grants and contributions every five years. The Treasury Board of Canada's Policy on Results (2016) defines such a review as a form of evaluation. An evaluation of AHHRI was previously completed in 2012-2013.
1.2 Program Profile
AHHRI originated from a commitment made by the Government of Canada at the Special Meeting of the First Ministers and Aboriginal Leaders in September 2004. Funding is provided through contribution agreements for activities to increase the number of First Nations, Inuit and Métis workers in the health care field, and to ensure that community-based workers are trained and certified to improve the quality and consistency of health care services provided in First Nations and Inuit communities.
Until the end of 2014-15, AHHRI was a component of a broader pan Canadian Health Human Resources Strategy and consisted of five components:
- bursaries and scholarships;
- training for community-based workers;
- promotion of health careers;
- post-secondary educational support programs; and
- health human resources planning, implementation and integration; and, capacity building and knowledge translation.
The AHHRI as well as the pan-Canadian Health Human Resource Strategy underwent program and funding changes as a result of the Government of Canada program review and deficit reduction strategy. As a result, in 2015, the AHHRI underwent a re-design to offer funding through two streams, with a concomitant reduction in overall program funding:
- Stream 1 (3.0 million/year): provides scholarships and bursaries to Indigenous students in post-secondary education programs leading to health careers. Scholarships and bursaries are offered to First Nations, Inuit and Métis students enrolled in health and dental studies at universities and colleges. The financial assistance is delivered by Indspire, an Indigenous‑led, registered national charity dedicated to advancing the educational outcomes of First Nations, Inuit and Métis peoples. Indspire distributes AHHRI funding through its Building Brighter Futures awards program.
- Stream 2 (1.5 million/year): provides funding for the training of community based health care workers and health managers working in health promotion and disease prevention in First Nations and Inuit communities. The training targets health workers employed in community, tribal council or tribal health authority who do not belong to either a regulated health profession (e.g., Registered Nurses) or a regulated allied health profession (e.g. occupational therapy). The funding is delivered by FNIHB regional offices, which consult with Indigenous communities and organizations to determine regional priorities for training.
1.3 Program Narrative
As shown in the logic model in Appendix A, AHHRI expected outcomes are:
Immediate outcomes:
- Indigenous people participate in post-secondary education leading to health careers; and
- Community-based workers are trained to improve the quality and consistency of health care services in First Nations and Inuit communities.
Intermediate outcomes:
- Greater capacity of community health workers and health managers working in First Nation and Inuit communities; and
- Indigenous people are working in the health sector.
The ultimate program outcome is that First Nations and Inuit are able to influence and/or control (design, deliver and manage) health programs and services.
1.4 Program Alignment and Resources
AHHRI was formally announced in Budget 2005 as a new investment of $100 million over five years and then renewed in March 2010 when the Initiative obtained $80 million from 2010‑11 to 2014-15. The program re-design in 2015 to two funding streams included a reduction in overall funding to approximately $5 million per year. As shown in Table 1, over the evaluation period due to the re-design of the program and reduced funding, annual expenditures decreased from approximately $13.6 million in 2013‑14 to approximately $5.8 million in 2017‑18. This reduction in funding occurred in parallel with a steady increase in the number of applicants for AHHRI scholarship and bursaries (see Section 3.6 of this report for more details).
| Expenditures | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 | Total |
|---|---|---|---|---|---|---|
| Salaries | 741 | 1,218 | 869 | 663 | 677 | 4,168 |
| Operations and Maintenance | 54 | 160 | 181 | 147 | 133 | 675 |
| Contributions | 12,789 | 6,039 | 4,703 | 4,842 | 4,992 | 33,365 |
| Total: AHHRI | 13,584 | 7,417 | 5,753 | 5,652 | 5,802 | 38,208 |
Source: Financial data provided by the Chief Financial Officer Branch, Health Canada |
||||||
Overall, AHHRI represents a relatively small investment. However, as discussed in Section 3.5 of this report, it coexists alongside a variety of other governmental and non-governmental programs, that also aim to help Indigenous people pursue post-secondary education or that provide funding for the training of health workers in Indigenous communities.
2. Evaluation Description
2.1 Evaluation Scope, Approach and Design
The evaluation focused on Stream 1 and 2 activities from April 2013 to March 2018. It covered all Stream 1 scholarships and bursaries offered across Canada and Stream 2 training delivered in all FNIHB regions except British Columbia, where responsibilities for federal health on‑reserve programs have been transferred to the First Nations Health Authority through the 2011 British Columbia Tripartite Framework Agreement on First Nation Health Governance.
The evaluation's design and data collection methods were guided by Treasury Board's Policy on Results (2016). The Assembly of First Nations (AFN) and Inuit Tapiriit Kanatami (ITK) were consulted during the development of the evaluation framework and were provided with an opportunity to review and comment on the evaluation instruments, the preliminary findings, and the evaluation report.
Recognizing that AHHRI represents a small program investment, the evaluation team opted for a calibrated approach that focused on the use of qualitative data and existing monitoring data collected by Indspire, the recipient-organization responsible for delivering Stream 1 scholarships and bursaries. Overall, the evaluation employed the following:
- a review of documents and files, including internal documents, the 2013 evaluation, program and regional reports and financial data;
- a review of Indspire annual monitoring reports and surveys of recipients;
- a review of published literature on Indigenous health human resources; and
- interviews with 31 key informants from FNIHB national and regional program staff, associations of Indigenous health professionals; national Indigenous organizations; university student support services; and regional and community-based Indigenous health services organizations.
The use of multiple lines of evidence and triangulation increased the reliability and validity of the evaluation findings and conclusions.
2.2 Limitations and Mitigation Strategies
Most evaluations face constraints that may affect the reliability of findings. Table 2 outlines the limitations encountered during this evaluation as well as the mitigation strategies put in place to increase the reliability of the evaluation findings. Overall, due to the use of a calibrated approach and, challenges related to availability of data and the context in which this program operates (i.e., small program exist alongside a multitude of similar programs), this evaluation is not able to provide clear answers about the impacts AHHRI had in terms of helping Indigenous people to work in health careers and of increasing the capacity of community health workers. It does, however, provide various examples of the benefits of AHHRI for health students and First Nations and Inuit communities.
| Limitation | Impact | Mitigation Strategy |
|---|---|---|
| Performance data on the intermediate and long-term outcomes of Stream 1 was limited (i.e., covered only a cohort of Stream 1 recipients and only captured their employment situation at one point in time after their participation). | The evaluation provides limited information on achievement of intermediate outcomes and could not assess the achievement of the long-term outcome for Stream 1. | Results of recipient surveys conducted by Indspire provide some proxy information on achievement of intermediate outcomes. This data was complemented with information provided by key informant interviews. |
| The evaluation could not access consistent performance data on outcomes of Stream 2 projects across Canada. | The evaluation does not provide an exhaustive national-level assessment of possible benefits and challenges related to Stream 2 funding. | A sample of project reports was used to assess the type of activities funded under Stream 2 and possible benefits resulting from these activities. This information was complemented by views of key informants from different regions and organisations in order to capture a variety of perspectives about Stream 2. |
3. Findings
3.1 Relevance: Continued Need for the Program
There is a continued need for more Indigenous health workers who can contribute to improving the quality of services for Indigenous People.
The recent evaluation of the FNIHB Clinical and Client Care Program found that there is an insufficient level of cultural sensitivity in the delivery of health care. As reported in the literature, internal documents and key informants, the lack of cultural considerations in the provision of health care can manifest itself, among other things, through difficulty in accessing traditional medicine, difficulty in receiving care in Indigenous languages, racism toward Indigenous people or perception that services are culturally unsafe. This lack of cultural consideration or sensitivity can represent a real or perceived barrier to accessing health care for Indigenous people. For example, research has shown that racism against Indigenous peoples can lead them to avoid using health care in anticipation that they may be victimizedFootnote 1.
AHHRI supports the greater inclusion of cultural competencies in health care through its objective of increasing the number of Indigenous health workers. Program documents, the literatureFootnote 2 and a few key informants from both FNIHB and regional or community Indigenous originations reported that Indigenous health workers with cultural and community insight can help ensure a greater inclusion of cultural considerations in the provision of health care. However, Indigenous people continue to be underrepresented in health occupations. As outlined in the 2016 Census data, the proportion of Indigenous people working in health occupations is two percentage points lower than the proportion of non-Indigenous people working in those same occupations (i.e., five percent of Indigenous people employed in 2015. worked in health occupations as compared to seven percent of the non-Indigenous population)Footnote 3 This suggests that there is a continued need to support Indigenous people to train for health occupations.
There is a need to address financial barriers to accessing health studies
Indigenous people continue to experience lower educational attainment than the non Indigenous population. For example, the 2016 Census data show that 34 percent of the Indigenous identity population aged 15 years and older had less than a high school certificate/diploma compared to 18 percent for the non-Indigenous populationFootnote 4. As explained in an Indspire documentFootnote 5, Indigenous people are underrepresented in all areas of education and face numerous barriers to accessing studies. These barriers can be academic, cultural, personal, emotional, financial or, related to language or home situation.Footnote 6
According to some key informants from Indigenous organisations and university support services, the provision of financial assistance can help address the financial barriers faced by Indigenous students. Reasons provided by key informants are that the student’s family may often not have the financial means to support the students, and that demands related to the studies can limit the ability of students to work part-time while attending classes. Similarly, health career students who received financial assistance through Indspire reported that financial burden is the second most significant barrier they faced after fatigue and stress.Footnote 7
There is also a need to continue developing the capacity of First Nations and Inuit community health workers
A few key informants from FNIHB mentioned that First Nations and Inuit communities (especially those in remote or isolated regions) often face challenges in terms of offering consistent health care services. As explained by key informants, this challenge may be due to difficulty in recruiting or retaining workers. Furthermore, key informants from FNIHB, regional/community Indigenous organisations and Indigenous health associations noted a need to increase the number of health workers in areas such as nursing, midwifery, health addiction, mental health, early childhood education, community support, dentistry and health care management.
Program documents and many key informants from regional and community Indigenous organisations reported the need within Indigenous communities for more skilled and competent health workers. In fact, a few key informants from regional and community organisations explained that developing the skills and capacity of currently employed workers is one of the biggest challenges they are facing. AHHRI can contribute to addressing those needs through both Stream 1 and Stream 2 activities.
3.2 Relevance: Alignment with Indigenous Priorities
AHHRI's objectives align with Indigenous health priorities identified in recent calls for action from Indigenous governance organisations. Program objectives also align with priorities identified by Indigenous representatives interviewed for this evaluation.
The AFN's 2017 First Nations Health Transformation Agenda recognized the need to continue addressing shortages of health professionals, Indigenous representation in the health workforce, cultural safety and competency, educational barriers at the pre- and post-secondary level, pay equity, and continuing professional education and peer support.Footnote 8One of the AFN's recommendations included a call to increase AHHRI funding to its 2005-2010 level.
The ITK 2011-2021 Inuit Health Human Resources Framework & Action PlanFootnote 9 and its 2017 report An Inuit-Specific Approach to the Canadian Health AccordFootnote 10 also outlined the need to address shortages of health professionals in communities, barriers to education, recruitment and retention, and the need to support community workers.
Both the AFN and ITK documents contain recommendations that are aligned with the 2015 Truth and Reconciliation Commission of Canada's Final Report, which through its Calls to Action number 23 called all levels of government toFootnote 11:
- Increase the number of Aboriginal professionals working in the health-care field;
- Ensure the retention of Aboriginal health-care providers in Aboriginal communities; and
- Provide cultural competency training for all health care professionals.
The principle underlying the issues and actions identified in the Truth and Reconciliation Commission and in the AFN and ITK documents is the need to empower Indigenous communities to achieve greater control over the determinants of community and individual health and well-being. Read together, these documents make a series of recommendations in the following areas, which are all aligned to AHHRI's objectives:
- Increasing the number of Indigenous people studying for and working in health careers, including addressing financial barriers to education;
- Increasing the capacity of health workers in Indigenous communities through improved access to training; and,
- Retaining health workers in Indigenous communities.
As well, a 2016 presentation by the Métis National Council identified a need for specific measures to support the development and implementation of specific health human resources strategies for First Nations, Inuit and Métis.Footnote 12
Finally, many Indigenous key informants interviewed for the evaluation identified priorities around increasing the ability of communities to manage and control funding and priorities for health services. They also reported priorities around building the capacity of health services staff.
3.3 Relevance: Alignment with Federal Priorities
AHHRI aligns with federal priorities to increase the representation of Indigenous people in the Canadian workforce, to support Indigenous post-secondary education and skills development and to improve the delivery of health services in Indigenous communities. Various priority setting or policy documents issued over the last couple of years consistently reiterated those priorities.
The Government of Canada has accepted the Truth and Reconciliation's Calls to Action and the United Nations Declaration of the Rights of Indigenous People with the principles of increasing the autonomy and authority of Indigenous communities, bettering access to health care services and improving health outcomes of Indigenous populations.
In addition, over the last few years, the Government of Canada has continued to support Indigenous communities to control and influence their health services through various initiatives. These include the 2011 Tripartite Framework Agreement on First Nations Health Governance that led to the creation of the First Nations Health Authority in British Columbia and the signing of the Charter of Relationship Principles Governing Health System Transformation in Nishnawbe Aski Nation Territory in 2017. This agreement includes the objective of increasing community capacity to plan and deliver health services.Footnote 13
Furthermore, the 2017 federal/provincial/territorial negotiations on federal funding for health care services led all parties to endorse a Common Statement of Principles on Shared Health Priorities.Footnote 14 This included a commitment for federal/provincial/territorial governments to work with First Nations, Inuit and Métis to improve health services and outcomes, respecting Indigenous health priorities as identified in the First Nations Health Transformation Agenda, An Inuit-Specific Approach to the Canadian Health Accord and the Métis health agenda.
Federal budgets from the last five years, as well as the Ministerial mandate letters for Health Canada in 2015 and Indigenous Services Canada in 2017, include commitments to increase the representation of Indigenous people in the Canadian workforce, to support Indigenous post‑secondary education and skills development and to improve access, quality and safety of health services in Indigenous communities.
More recently, in January 2018, the Minister of Indigenous Services Canada reiterated the Department's priorities around improving Indigenous health outcomes and supporting the number of Indigenous people entering health careers.Footnote 15
3.4 Relevance: Alignment with Federal Roles and Responsibilities
The federal role in Indigenous health human resources stems from constitutional obligations for services for First Nations on-reserve and Inuit people. This role has been evolving in recognition of the shared jurisdictions for health and education and the objective of empowering Indigenous communities.
The federal role in providing health services to First Nations and Inuit communities has been evolving since the Indian Health Policy of 1979 with the growing recognition that Indigenous communities are best placed to identify needs and manage service delivery. In 2012, The First Nations and Inuit Health Branch Strategic Plan: A Shared Path to Improved HealthFootnote 16 recognized the complex, dynamic nature of the provision of health services for First Nations and Inuit, noting that a web of interdependent jurisdictional governance for health is shared by First Nations and Inuit, provincial/territorial and federal governments.
Likewise, the federal government has responsibility for elementary and secondary education in First Nations communities and has taken up a role in supporting post-secondary education and skills training for Indigenous people.
The Government of Canada's role in supporting health services in Indigenous communities and in providing support for post-secondary education for Indigenous students has been reiterated recently in the 2017 Ministerial mandate letter for Indigenous Services Canada.
3.5 Relevance: Complementarity or Duplication of Efforts
While a variety of financial assistance opportunities exist to support Indigenous post secondary students, they do not appear to duplicate grants and scholarships offered under AHHRI Stream 1. Other programs are more targeted to specific groups of students or geographic areas. Likewise, for Stream 2, although other programs support training of health workers in communities, there is no clear evidence of duplication since they tend to target job specific requirements or competencies.
3.5.1 Stream 1 (Scholarships and Bursaries)
Although scholarships and bursaries provided under AHHRI Stream 1 exist alongside a variety of other supports offered by the federal government and non-governmental organisations, the evaluation has not found examples of similar programs delivered by provincial and territorial governments. The AHHRI application is designed to ensure that AHHRI complements other funding available, so it is possible that students have received funding from other programs in addition to the AHHRI financial assistance. However, the evaluators did not access data on the proportion of AHHRI recipients that have received funding from other financial assistance programs.
At the federal level, Indigenous Services Canada provides the Postsecondary Student Support Program for First Nations and Inuit land claims organizations to distribute to their members, but it is not focused on any particular area of study, such as health careers. In addition, it is not available to non-status First Nations or membership in a First Nations band, Inuit who do not have membership in an Inuit land claim, or Métis.
Employment and Social Development Canada delivers the Aboriginal Skills and Employment Training Strategy, which provides financial assistance for training. However, it is targeted to Indigenous people who are unemployed, underemployed or require skills development. The Strategy is not specific to health careers and aims to meet labour market demand. Employment and Social Development Canada also funds the Canada Student Loan and Grant Program, which is not specific to Indigenous students, but is open to Indigenous students to apply.
There are a variety of scholarships and bursaries provided by universities or private and non for profit organisations intended to support Indigenous students undertaking health studies. In particular, the Indigenous Services Canada online Indigenous Bursaries Search Tool lists 58 awardsFootnote 17 specific to the category of Health Careers and Services, including the AHHRI scholarships and bursaries. However, unlike AHHRI, these scholarships and bursaries are often targeted to very specific groups of health students and limited to a small number of awards, for example:
- The University of Manitoba’s Joan and Dean Sandham Scholarship in Aboriginal Health Professional Leadership is offered to First Nations, Métis and Inuit students who have completed an undergraduate program in Medicine or Nursing and are pursuing further degree studies that will specifically enhance and develop their leadership skills.
- Baxter Corporation - Jean Goodwill Scholarship administered by the Canadian Indigenous Nurses Association provides two scholarships annually of $2500 each to applicants of Indigenous ancestry for specialized training in nursing, and for those enrolled in a Bachelor level nursing program who agree to secure employment in Indigenous communities.
In addition, other programs offered by Indigenous organisations are not listed in the Indigenous Bursaries Search Tool, including:
- The National Indian Brotherhood Trust funding, which is available to groups and individuals under the terms of the Indian Residential Schools Settlement Agreement.Footnote 18
- The Gabriel Dumont Institute in Saskatchewan, which offers one award annually for Métis students enrolled in Dumont Technical Institute Licensed Practical Nursing Program in Regina. Footnote 19
Overall, there is a large variety of financial supports, which target various groups of Indigenous students. However, key informants generally noted that existing funding falls short of demand. As well, as discussed in Section 3.6.1, monitoring data from Indspire suggest that available funding, including Stream 1, covers a relatively limited share of student’s financial needs. AHHRI Stream 1 is designed to minimize the risk of duplication with other programs since the application form requires students to report other sources of funding and the size of the scholarships and bursaries is determined based on the financial needs not already covered by other sources of funding.
3.5.2 Stream 2 (Training for community-based workers and managers)
Similarly, for Stream 2, although other programs support training of health workers in communities, there is no clear evidence of duplication, as they tend to target different areas (e.g., job specific requirements or specific competencies) or categories of health workers.
Other FNIHB programs include training components, which can support the development of unregulated health workers in the communities. Key examples include:
- The Home and Community Care Program supports training for health professionals and community workers in areas such as chronic disease and acute care management, and in health promotion and diabetes prevention.
- The eHealth Infostructure Program includes a training component to prepare staff to use technologies such as telehealth equipment and electronic health record systems.
- The National Native Alcohol and Drug Abuse Program supports the training of community based addictions counsellors and has a third-party certification process, providing a means to increase skills and take on more senior roles.
In addition to these FNIHB programs, a few key informants identified examples of training offered by provinces and territories to support community health workers in adopting health electronic records. In one instance, AHHRI was used to complement funding provided by the territory in order to increase the number of participants who could benefit from that type of training.
Overall, key informants from FNIHB and Indigenous regional or community organisations mentioned that Stream 2 funding complements other FNIHB and provincial/territorial training efforts.
3.6 Performance: Achievement of Stream 1 (Scholarships and Bursaries) Outcomes
3.6.1 Reach of Stream 1 Funding
The AHHRI Stream 1 scholarships and bursaries have contributed to helping approximately 765 Indigenous students per year to participate in post-secondary education in a health related field of study.
An analysis of annual monitoring data collected by Indspire, the recipient-organisation responsible for delivering AHHRI Stream 1 scholarships and bursaries,Footnote 20 shows that 3,061 health-field scholarships/bursaries were awarded to Indigenous health students over the 2013-14 to 2016-17 period. This represents an average of approximately 765 students per year (see Table 3). The average amount per award was $3,339 over the period.
The number of AHHRI applicants per year has grown steadily and significantly over the period; increasing from 809 applicants in 2013-14 to 1,120 in 2016-17. The number of actual recipients remained, however, fairly consistent over these years. As a result, the percentage of students who applied for Stream 1 scholarships and bursaries and were successful in obtaining funding steadily declined over the evaluation period.
| 2013-14 | 2014-15 | 2015-16 | 2016-17 | Total | |
|---|---|---|---|---|---|
| Number of applicants | 809 | 1,109 | 1,046 | 1,120 | 4,084 |
| Number of awards granted | 706 | 882 | 764 | 709 | 3,061 |
| Proportion of successful applicants | 88% | 79% | 73% | 63% | n/a |
| Average amount per award | $4,160 | $2,835 | $3,148 | $3,357 | n/a |
Source: Annual monitoring data provided by Indspire |
|||||
As shown in Table 4, on average, 80 percent of recipients were women. Over the evaluation period, most recipients were studying in nursing-related field followed by medicine and human kinetics. However, the proportion of recipients enrolled in nursing related studies and medicine declined fairly steadily over the evaluation period. Factors explaining such a decrease are not known.
| 2013-14 | 2014-15 | 2015-16 | 2016-17 | |
|---|---|---|---|---|
| Number of Recipients | 706 | 882 | 764 | 709 |
| Sex | ||||
| Male | n/a | 20% | 21% | 18% |
| Female | n/a | 80% | 79% | 82% |
| Three Largest Fields of Study | ||||
| Nursing-related | 48% | 50% | 45% | 41% |
| Medicine | 20% | 15% | 16% | 14% |
| Human Kinetics | 8% | 9% | 10% | 10% |
| Indigenous Affiliation | ||||
| First Nations | 50% | 50% | 47% | 48% |
| Non-status First Nations | 0% | 3% | 4% | 5% |
| Inuit | 2% | 1% | 2% | 3% |
| Métis | 48% | 46% | 47% | 44% |
| Year of Study | ||||
| Year 1 | 31% | 33% | 34% | 35% |
| Year 2 | 29% | 30% | 31% | 29% |
| Year 3 | 22% | 21% | 22% | 19% |
| Year 4 and beyond | 19% | 16% | 13% | 17% |
Source: Annual monitoring data provided by Indspire |
||||
Over the evaluation period, the vast majority of recipients were either from First Nations (48 percent to 50 percent) or from Métis population (44 percent to 48 percent). Inuit and individuals identifying as non-status First Nations represented a minority of recipients but their share among the total number of recipients steadily increased over the period. Overall, the proportion of Métis receiving AHHRI awards is relatively high compared to their representation among the Indigenous population in Canada (i.e., Metis represented 35 percent of individuals reporting Aboriginal identity in the 2016 Census).Footnote 21 The evaluation has not investigated the reasons behind the high representation of Métis among AHHRI recipients. However, considering that the Métis population is not eligible to receive funding from programs like the Postsecondary Student Support Program, it may be useful to undertake more analysis in the future to determine if such factors contribute to the higher uptake of AHHRI by Métis students.
Indspire scholarships/bursaries are granted on an annual basis, and students can re-apply. Overall, approximately one third of recipients were in their first year of study while slightly less were in their second year (29 percent to 31 percent) and about one fifth were in their third year.
Lastly, as shown in Table 5, Quebec and the northern region have the lowest proportion of recipients while Ontario has the highest. In comparison with the distribution of Indigenous identity population in Canada identified in 2016 Census, students from Saskatchewan and Atlantic have a relatively high representation among Stream 1 recipients while those from Quebec and Alberta have a relatively low representation. Factors explaining the uptake of AHHRI funding by recipients from these regions were not examined in the evaluation.
| Region | Distribution of Stream 1 Recipients by Region 2015-16 | Distribution of Indigenous identity Population in Canada, 2016 | Difference in Percentage Points |
|---|---|---|---|
| British Columbia | 15% | 16% | -1 |
| Alberta | 10% | 15% | -5 |
| Saskatchewan | 16% | 10% | +6 |
| Manitoba | 17% | 13% | +4 |
| Ontario | 23% | 22% | +1 |
| Quebec | 5% | 11% | -6 |
| Atlantic | 13% | 8% | +5 |
| Northern | 2% | 4% | -2 |
Source: Insdpire monitoring data and Statistics Canada 2016 Census. |
|||
3.6.2 Ease of Application Process
Some key informants noted that the Indspire bursaries and scholarships application process can be challenging for students to complete.
The application process for Stream 1 scholarships and bursaries requires applicants to submit a set of documentation such as:
- proof of Indigenous status;
- education funding letter (requiring First Nations and Inuit applicants to detail any financial support from their community);
- proof of enrollment in a full-time academic program;
- proof of community involvement; and,
- a letter of introduction detailing ties to community and culture, academic challenges and successes, and a career vision.
Applications are scored on different criteria like volunteerism, academic achievement, as well as level of financial need. Some key informants from community or regional Indigenous organisations and university support services reported that the Indspire application process is quite challenging for students to complete. Success depends on the skills and resources of the applicant to seek appropriate documentation (e.g., letters of support, proof of community involvement etc.,) and to write an articulate letter of introduction. Key informants, including those from university support services, explained that students often need help to complete the application. In some instances, universities provide application workshops as well as individual coaching on how to complete the application. Indspire also provides support, including a Webinar to help students apply. Overall, some key informants reported that the effort required to apply is often very high relative to the financial amounts granted.
3.6.3 Level of Awareness of Stream 1 Scholarship and Bursary
While the number of Stream 1 applicants has increased significantly in the last few years, and although Indspire and universities are conducting outreach activities to promote post secondary education and available scholarships and bursaries, many key informants reported that awareness within communities about Stream 1 awards could be improved.
Key informants and the Indspire website noted that, as part of its efforts to promote educational achievement for Indigenous people, Indspire undertakes awareness-raising activities such as an annual Indspire Awards ceremony.Footnote 22 As well, it also provides training to previous award recipients so they can assist applicants for future awards and mentor high school students who may be interested in post-secondary education.Footnote 23 Two university-based key informants reported that they promote funding opportunities, including those from Indspire, to registered students who identify as Indigenous.
Despite these efforts, many key informants from regional and community-based health services organizations and FNIHB reported that they had not observed much outreach in their regions. They stated that awareness of the Indspire scholarships and bursaries in the Indigenous communities that they serve could be improved. Moreover, a few key informants, including university support services, mentioned that it is difficult to find comprehensive information on the Indspire awards and other scholarships and bursaries available. A suggestion heard in the evaluation is to have a centralized application system that could allow students to apply for multiple awards at once.
3.6.4 Contribution of Stream 1 Funding to Pursue Studies
The financial assistance provided by AHHRI Stream 1 covers approximately 17 percent of student financial needs and is seen by students as helping to relieve financial stress.
Indspire annual monitoring data show that the AHHRI funding granted to students averaged $3,339 per year and covered an average of 17 percent of the total financial needs reported by applicants on the application form. The share of financial needs covered did not vary significantly between 2014-15 and 2016-17 (i.e., remained in the 14 percent to 16.5 percent range). There was however a significant difference between those years and the 2013 14 recipients whom had about 45.5 percent of their financial needs covered by the AHHRI scholarships and bursaries. The amount of financial assistance requested by the 2014 15 to 2016-17 recipients varied between $17,200 and $22,200 as compared to about $9,100 for the 2013-14 recipients. It is this increase in the level of financial assistance requested that mainly explains the decrease in the share of financial needs covered by AHHRI funding.
The application form defines financial needs as the difference between the costs incurred by the students (e.g., tuition, books, living costs etc.) and the financial resources they were able to access (e.g., other financial assistance, employment income, etc.). In this context, it appears that a significant portion of students’ financial needs remain unmet by the available sources of funding. However, it is not known to what extent students were able to access other sources of financial assistance after submitting their Stream 1 application.
Although the funding covers a relatively limited proportion of student financial needs, Stream 1 recipients reported that the awards helped them to relieve stress and focus on their studies. Specifically, over three-quarters of Stream 1 scholarship and bursary recipients surveyed by Indspire (78 percent in 2012-13Footnote 24 and 84 percent in 2013-14Footnote 25) said that the award helped to relieve stress. Related to this, 78 percent of respondents in 2012-13 and 2013-14 said that the awards helped with living expenses, and over half agreed that it allowed them to focus on their studies and to achieve better marks (65 percent in 2012-13 and 72 percent in 2013-14).
A few key informants from communities and university support services also reported that that the funding was a key deciding factor in accessing and completing post-secondary education. Key informants from community/regional organisations noted that Stream 1 funding is appreciated by the recipients as it helps address some of their financial needs, but that a larger part of their needs are still unmet, forcing many to seek additional funding, take part-time jobs or to cope with poverty.
3.6.5 Barriers to Accessing Studies
Key informants frequently indicated that many Indigenous people face a significant barrier to accessing post-secondary health studies because they have not completed the prerequisites (e.g., math or science).
Program documents, the literatureFootnote 26 and many key informants reported that Indigenous students often lack academic prerequisites and skills necessary to enter post-secondary studies, as well as a career goal that would serve to inspire their studies. For students who wish to enroll in health-related post-secondary programs, upgrading is often required in the areas of math, science and reading/writing skills. Some key informants from FNIHB, community or regional organisations or association of health professionals emphasised that students need to be reached early to help them develop a career vision and provide them appropriate supports to build the prerequisites to realize that vision.
Prior to 2015-16, AHHRI funds could be used to support health career promotion. As shown in AHHRI project reports, funded activities of this type primarily consisted of participating in career fairs or other community events like powwows to speak with interested participants and distribute materials.
Since 2015-16, career promotion activities are no longer supported under the AHHRI. However, other organisations such as Insdpire are undertaking some outreach activities to promote post secondary studies. As well, a few key informants from community or regional organisations indicated that some communities continue to promote health careers without support from AHHRI. Examples include youth-oriented career fairs that cover many different employment sectors or the provision of summer job experiences in health services for high school and post secondary students. As well, a series of other examples of pre-health studies supports were identified in project reports, websites and key informant interviews. Some of these have received AHHRI funding in the past.
The evaluation did not examine the extent to which these initiatives fill the gap left from the 2015 change in AHHRI’s scope. However, various key informants interviewed for the evaluation frequently reported a continued need to do more in terms of helping students to acquire the prerequisites to enter university programs in the health field and to promote health careers.
Overall, evaluation findings suggest that AHHRI Stream 1 is more focussed on helping students to complete their health studies, as opposed to increasing the number of students enrolling in health studies.
3.6.6 Level of Employment in Health Sector after Completing Studies
After graduating, most Stream 1 scholarship and bursary recipients were employed in an area where their health studies was relevant and were serving Indigenous populations as part of their job.
A 2015 survey of previous Indspire recipientsFootnote 27 shows that, of 249 respondents who graduated from a health-related field, 88 percent were employed after completing their studies. Of those, 93 percent indicated that their health-field education was relevant for their employment. Data available do not show what proportion remained employed in the field in the medium to long term after graduation. As well, at the time of the evaluation, there was no data on the employment of the more recent cohort of health study graduates.
Another expected outcome of AHHRI is the improvement of the capacity of health workers in Indigenous communities. The employment of graduates of post-secondary health-related programs in Indigenous communities may contribute to this outcome. In that respect, the majority (80 percent) of respondents to the 2015 survey stated that they were serving Indigenous populations as part of their work, however, the survey did not indicate if they were working in an Indigenous community.
While there is no data available on the rate of return of Stream 1 recipients to their own communities, key informants and Indspire survey respondents from 2012-13 identified several barriers impacting the return of graduates to Indigenous communities. Barriers commonly identified by key informants and 2012-2013 Indspire survey respondents include:Footnote 28
- uncertainties of finding employment and a lack of opportunities for advancement;
- difficulties of re-integrating into the community after having lived outside of the community for an extended period of time;
- requirements to move or travel to serve remote communities;
- higher wages in similar positions outside of Indigenous communities (e.g., in the provincial health system);
- lack of Indigenous language abilities; and
- lack of housing in some communities.
3.7 Performance: Achievement of Stream 2 (Training for community based health workers and managers) Outcomes
3.7.1 Training activities funded under AHHRI
AHHRI Stream 2 funding has supported training for community-based workers in a variety of domains such as training on addictions and mental health counselling, early childhood education, certification for health managers and personal support worker.
Stream 2 activities have resulted in a variety of training opportunities being offered across all FNIHB regions.Footnote 29 As shown in the examples identified below from program documents and key informant interviews, Stream 2 funding was used to fund a variety of training to support workers in the area of health practices, such as fetal alcohol spectrum disorder, mental wellness, grief and trauma, addiction, personal support worker, social service, native community worker and community health manager. Example of specific training organised in different FNIHB regions include:
- in Alberta, tuition was funded for Community Health Workers to enroll in a college-based Community Health Promotion certificate program, offered via distance education to allow students to maintain their employment;
- in Saskatchewan, Certified Community Wellness training was organized in 2013-14. Diabetes education was also offered to Community Health Representatives and Personal Support Workers in 2015-16 and 2016-17;
- in Ontario, funding was directed to First Nations education institutes to offer accredited post secondary programs for First Nations health workers in partnership with community colleges in a variety of domains such as Early Childhood Education, Personal Support Worker, and addictions counselling;
- in Quebec, AHHRI funding was used by the Cree Board of Health to train Community Health Representatives and by the Centre de développement de la formation de la main d’oeuvre Huron-Wendat (Wendake) for training Personal Support Workers in 2013-14; and
- in Yukon, AHHRI funding was used for training on electronic health record management for community workers in 2015-16.
Beyond training community health workers, AHHRI funding was used in a few instances to support short-term certification required in the workplaces (e.g. day care centres) such as First Aid/CPR (Cardiopulmonary Resuscitation), food safety and Workplace Hazardous Materials Information System.
The evaluation also found a few examples of Stream 2 funding being used to assist community worker capacity-building for other FNIHB programs such as Aboriginal Head Start and Home and Community Care.
3.7.2 Contribution to increasing the capacity of health and/or community workers
Stream 2 funding contributed to increasing the qualifications of health workers in communities and helped to improve health services.
According to program documents and key informants, training activities funded under Stream 2 contributed to raising the qualifications of health workers, helping them to gain a better understanding of the health issues faced by their communities and their role in responding to them. The training supplemented on-the-job learning and helped community workers gain more confidence, resiliency and flexibility. It is seen as contributing to raising the quantity and quality of services provided to the community.
A specific example of how AHHRI was used to support community health workers was found in Alberta. The pre-2013 AHHRI program was used to develop the job descriptions and competencies for Community Health Representatives. These Community Health Representatives occupy one of the core non-regulated positions on health teams in First Nations and Inuit communities and fulfill a myriad of responsibilities, including health educator, interpreter and patient advocate. A First Nations Community Health Promotion training program was established to train Community Health Representatives and AHHRI Stream 2 funding in Alberta is being used to fund the participation of Community Health Representatives in this program.
Among other benefits, key informants explained that community workers trained with Stream 2 funding gained confidence in their abilities to pursue further training or post-secondary education. This can lead to opening up the possibility to move up within their organizations or to move into other related fields of employment, (e.g., using early child education training to take on a related role in a community’s Maternal and Child Health Care Program).
Although AHHRI aims to increase the capacity of health workers within First Nations and Inuit communities, key informants commented that trainees are likely to consider employment opportunities outside of their communities where wages are often higher (e.g. in provincial health care facilities, social services or education organizations). In this context, a few key informants noted that keeping workers with newly upgraded qualifications represents a challenge for some communities.
3.7.3 Contribution to achieving long-term outcome
There is a clear example of how the Stream 2 funding led to initiatives resulting in capacity building for First Nations communities.
The pre-2013 version of AHHRI helped to fund the creation of the First Nations Health Managers Association and the establishment of its certification program for health managers. While AHHRI Stream 2 no longer provides core funding to the FNMHA, AHHRI funding continues to be used to help health managers in First Nations communities to pursue certification offered by the Association. A couple of key informants from community or regional organisations, health professional associations and FNIHB spoke about the benefit of this initiative. In particular, it was mentioned that the First Nations Health Manager designation has contributed to improving the management capacity within First Nations communities and the growth of a peer network. In addition, communities are now increasingly looking to hire health professionals and health administrators with this designation. The training is also seen as helping First Nations communities to move from fixed to more flexible funding arrangements.
3.7.4 Challenges with the design and delivery of Stream 2
There were some challenges with the design and delivery of Stream 2, primarily in relation to the amount of funding, the eligibility criteria and a lack of clarity on Stream 2 guidelines.
A couple of FNIHB and community or regional organisation key informants indicated that the $1.5 million annual Stream 2 budget is split between seven regions, leaving communities and regional groups with a relatively small budget to offer training.
This is seen as resulting in an increasing number of unmet needs within the communities. Some key informants from community or regional organisations noted that in order to make the best use of limited funds, some regional groups decided to use Stream 2 to support only one type of training while other priorities could not be addressed. For example, one community key informant noted that an AHHRI-funded Community Health Representative training program was no longer supported in their region although it is still seen as being needed.
In addition, key informants from community or regional based organisations identified various training needs that could not be addressed due to the Stream 2 eligibility criteria, which target non regulated workers and community-based workers in health promotion and disease prevention. Examples of unmet training needs mentioned by key informants included:
- foundational computer/office administration skills;
- academic upgrading for First Nations and Inuit community members;
- continuing education for any core staff such as nurses, licensed practical nurses or social workers;
- development of cultural competencies, traditional healing or soft skill development (e.g., self esteem and team building); and
- ongoing mentoring of staff about First Nations and Inuit ways of learning and to support career progression into leadership positions, e.g., for nurses.
A lack of clarity around how to interpret program guidelines was also noted by some community based key informants. This may have led to the refusal of some training projects that may have actually been eligible. According to key informants, FNIHB consulted with First Nations and Inuit communities and organizations to update the Stream 2 guidelines in 2016. The intention was to simplify the guidelines and make them more responsive to community needs, especially with northern and Inuit communities. However, as noted by key informants in some regions, a lack of clarity around how to interpret the guidelines remains.
Finally, another challenge identified in the evaluation is a lack of awareness of AHHRI funding among health managers. According to a survey of health managers conducted for the recent Clinical and Client Care Program evaluation, only about half were aware that AHHRI existed and very few had used the program.
4. Efficiency
4.1 Program Budget and Expenditures
AHHRI expenditures have decreased from approximately $13.6 million in 2013-14 to $5.8 million in 2017-18. Actual spending on Stream 1 and 2 contribution funding approximated $3.5 and $1.5 million respectively in the last two years of the evaluation period.
As shown in Table 6, AHHRI expenditures have decreased over the evaluation period and planned spending has been reallocated to other program priorities within FNIHB. Program spending has remained relatively consistent since 2015-2016 and ranged between $5.7 and $5.8 million per year.
| Expenditure type | Planned ($) | Expenditures ($)a | Variance ($)b | % budget spent |
|---|---|---|---|---|
| 2013-2014 | ||||
| Salaries | n/a | 740,815 | n/a | n/a |
| Operations and Maintenance | n/a | 54,151 | n/a | n/a |
| Contributions | ||||
| AHHRI Increase Health Care Workers (Stream 1) | n/a | 2,846,692 | n/a | n/a |
| AHHRI Training (Stream 2) | n/a | 2,916,834 | n/a | n/a |
| Health Careers | n/a | 5,039,052 | n/a | n/a |
| HHR - Policy and Program Development | n/a | 1,986,489 | n/a | n/a |
| Total Contributions | n/a | 12,789,067 | n/a | n/a |
| Total | n/a | 13,584,033 | n/a | n/a |
| 2014-2015 | ||||
| Salaries | 1,086,081 | 1,217,927 | 131,846 | 112% |
| Operations and Maintenance | 140,738 | 160,328 | 19,590 | 114% |
| Contributions | ||||
| AHHRI Increase Health Care Workers (Stream 1) | n/a | 1,200,200 | n/a | n/a |
| AHHRI Training (Stream 2) | n/a | 1,002,965 | n/a | n/a |
| Health Careers | n/a | 3,635,587 | n/a | n/a |
| HHR - Policy and Program Development | n/a | 200,000 | n/a | n/a |
| Total Contributions | 8,319,405 | 6,038,752 | (2,280,653) | 73% |
| Total | 9,546,224 | 7,417,007 | (2,129,217) | 78% |
| 2015-2016 | ||||
| Salaries | 1,014,754 | 869,138 | (145,616) | 86% |
| Operations and Maintenance | 677,637 | 181,280 | (496,357) | 27% |
| Contributions | ||||
| AHHRI Increase Health Care Workers (Stream 1) | n/a | 635,000 | n/a | n/a |
| AHHRI Training (Stream 2) | n/a | 769,074 | n/a | n/a |
| Health Careers | n/a | 3,299,416 | n/a | n/a |
| HHR - Policy and Program Development | n/a | 0 | n/a | n/a |
| Total Contributions | 3,421,760 | 4,703,490 | 1,281,730 | 137% |
| Total | 5,114,151 | 5,753,908 | 639,757 | 113% |
| 2016-2017 | ||||
| Salaries | 1,030,306 | 663,165 | (367,141) | 64% |
| Operations and Maintenance | 673,796 | 146,614 | (527,182) | 22% |
| Contributions | ||||
| AHHRI Increase Health Care Workers (Stream 1) | n/a | 3,383,900 | n/a | n/a |
| AHHRI Training (Stream 2) | n/a | 1,458,051 | n/a | n/a |
| Health Careers | n/a | 0 | n/a | n/a |
| HHR - Policy and Program Development | n/a | 0 | n/a | n/a |
| Total Contributions | 8,108, 006 | 4,841,951 | (3,266,055) | 60% |
| Total | 9,812,108 | 5,651,730 | (4,160,378) | 58% |
| 2017-2018 | ||||
| Salaries | 1,046,425 | 676,541 | (369,884) | 65% |
| Operations and Maintenance | 681,810 | 132,691 | (549,119) | 19% |
| Contributions | ||||
| AHHRI Increase Health Care Workers (Stream 1) | n/a | 3,554,393 | n/a | n/a |
| AHHRI Training (Stream 2) | n/a | 1,437,493 | n/a | n/a |
| Health Careers | n/a | 0 | n/a | n/a |
| HHR - Policy and Program Development | n/a | 0 | n/a | n/a |
| Total Contributions | 8,306,418 | 4,991,886 | (3,314,532) | 60% |
| Total | 10,034,653 | 5,801,118 | (4,233,535) | 58% |
| Notes: Planned figures were not available for 2013-14 |
||||
4.2 Efficiency of AHHRI Program Delivery
4.2.1 Use of third-party delivery of Stream 1
Approximately 80 percent of the contributions provided to Indspire were redistributed in scholarships and bursaries. Considering that Indspire is actively engaged in outreach activities and promoting studies, the delivery of Stream 1 through this organisation allows some leveraging of resources, which can contribute to achieving AHHRI objective.
The 2015-16 program data demonstrated that, of the contributions provided to Indspire, 80 percent was directly redistributed to students in scholarships and bursaries. While actual amounts for the remaining 20 percent of expenditures are unknown, budget documents outline that the remaining funds were to be used for outreach and marketing (approximately one percent); monitoring and tracking (approximately one percent) and the balance for staffing and administration costs (approximately 18 percent).
In comparison, a 2016 evaluation of the Canadian Institutes of Health Research's Canada Graduate Scholarships program demonstrated that the average overhead cost was 1.8 percent, but the report noted that this was underestimated, as it did not include award administration costs borne by universities, or other similar costs.Footnote 30 As well, the 2007 annual report of the Canada Millennium Scholarship Foundation showed that the ratio of administrative costs compared to the total of awards distributed was seven percent.Footnote 31
It should be noted that Indspire undertakes outreach and marketing activities beyond activities funded under AHHRI Stream 1, which can contribute to achieving AHHRI's goal of increasing the number of Indigenous people working in health careers. In this way, program delivery through Indspire allows some leveraging of resources, which can contribute to AHHRI's objective. As previously discussed in this report, Indspire runs outreach programs to help elementary and secondary students build their vision of an education future and hosts an annual Awards gala that serves to publically recognize significant achievements among Indigenous people across Canada. AHHRI contributed funding in 2015-16 and 2016-17 to the Indspire Awards gala.
4.2.2 Coordination of Stream 2 programming
Practices have been put in place in FNIHB regions to coordinate decision making around allocation of Stream 2 funding with First Nations and Inuit organisations or provinces and territories. However, more could be done to coordinate the planning of AHHRI funding to better meet community health human resources needs.
Coordination between stakeholders on Stream 2 AHHRI funding decisions was observed in most regions. For example, in some regions, FNIHB and provincial government representatives were involved in funding decisions. In the northern region, as explained by some key informants, FNIHB held trilateral planning discussions with Inuit organizations and the Government of Nunavut (within the context of the Northern Wellness Agreement) in order to collectively identify priorities for how to use funding programs such as AHHRI.
In each of the Alberta, Manitoba, and Atlantic regions, annual Stream 2 funding was granted through a single contribution agreement in order to lower the administrative burden.
Although some level of coordination is taking place within the regions, a few internal and external key informants noted a lack of coordinated planning around the use of AHHRI funds to meet community health human resource needs and to ensure greater synergy with other FNIHB programs.
5. Conclusions and Recommendations
5.1 Conclusions
5.1.1 Relevance
There is a continued need for programming that aims to increase the number of Indigenous health workers, address financial barriers to accessing health studies and develop the capacity of First Nations and Inuit community health workers. AHHRI's objective is also aligned with Indigenous priorities around increasing the ability of communities to manage and control their health services; increasing the number of Indigenous people working in health careers and increasing the capacity of health workers in Indigenous communities. The Government of Canada has consistently reiterated similar priorities in recent years.
There are numerous examples of other programs that provide financial assistance to Indigenous students or training to First Nations and Inuit health workers. However, there is no clear evidence of duplication as those other programs target very specific groups or geographic locations.
5.1.2 Achievement of outcomes
Over the evaluation period, 3,016 AHHRI Stream 1 scholarships and bursaries have contributed to helping approximately 765 Indigenous students per year to participate in health post‑secondary studies. The financial assistance covered approximately 17 percent of student financial needs and is perceived as helping them to pursue their studies. Overall, the majority of students helped through AHHRI Stream 1 worked in a field related to their studies and served the Indigenous population as part of their work.
A few challenges were identified with respect to the design and delivery of Stream 1. In particular, the application process for the financial assistance is seen as being difficult for students to complete, especially for the level of funding provided. As well, a lack of prerequisite education is one of the biggest barriers faced by Indigenous people in terms of accessing health studies. Key informants identified a need to do more to help prospective student obtain the necessary skills to enroll in post‑secondary health programs. In this regard, evaluation findings suggest that AHHRI Stream 1 is focussed on helping students to complete their health studies as opposed to increasing the number of students enrolling in health studies.
AHHRI Stream 2 funding has supported the training for community-based workers in a variety of domains and is seen by key informants as helping to increase the qualifications of health workers in communities as well as contributing to improving health services. The evaluation has found compelling examples of how AHHRI has contributed to improving the capacity of First Nations communities to influence and control their health services. Specifically, AHHRI helped fund the creation of the First Nations Health Managers Association and the establishment of its certification program for health managers, which is seen as improving the management capacity within communities. Challenges related to the design and delivery of Stream 2 pertain to the limited amount of funding allocation compared to the existing needs, the eligibility criteria, which do not allow communities to get support for some training that could help increase the capacity of their health workers.
5.1.3 Efficiency
Approximately 80 percent of the contributions provided to Indspire were redistributed in scholarships and bursaries to students. In comparison, with other student financial assistance programs, overhead costs incurred by Indspire are high. However, considering that Indspire is actively engaged in outreach activities and promotion of studies, the delivery Stream 1 activities through this organisation allows some leveraging of resources, which can contribute to achieving AHHRI objectives.
Practices have been put in place in FNIHB regions to coordinate decision making around allocation of Stream 2 funding with First Nations and Inuit organisations or provinces and territories. However, more could be done to ensure that decisions around allocation of funding contribute to meeting community health resources needs.
5.2 Recommendations
The findings from this evaluation have led to the following two recommendations:
Recommendation 1:
Indigenous Services Canada should work with Indspire to increase accessibility to post‑secondary education in the health field by:
- Streamlining the application process to make it easier to complete;
- Developing supports to help students complete prerequisite courses; and
- Building on existing outreach activities to increase the promotion of health careers across communities.
Recommendation 2:
Indigenous Services Canada should ensure that training activities meet the needs of communities by:
- Engaging with communities to determine the best way to utilise the Stream 2 funding; and
- Increasing the coordination of AHHRI training activities with other similar ISC initiatives.
Appendix A– Logic Model
Logic Model for Aboriginal Health Human Resources Initiative
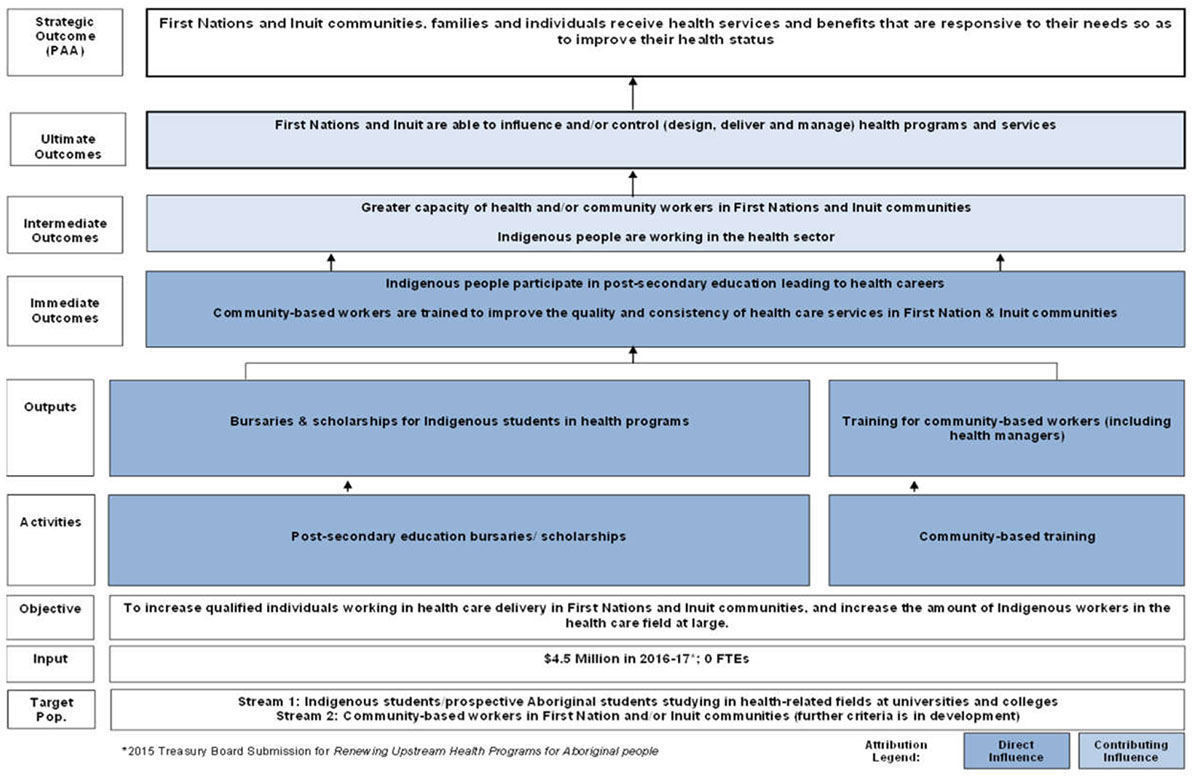
Text alternative for Appendix A– Logic Model for Aboriginal Health Human Resources Initiative
The Target Population of the initiative is broken down into two streams: Stream 1) Indigenous students/prospective Aboriginal students studying in health-related fields and colleges and universities; and, Stream 2) Community-based workers in First Nation and/or Inuit communities (further criteria is in development.)
The Input for the initiative $4.5 million in 2016-2017 and 0 Full-time Employees. (The figure of $4.5 million was taken from the Treasury Board Submission for "Renewing Upstream Health Program for Aboriginal People".)
The Objective of the initiative is listed as "To increase qualified individuals working in healthcare delivery in First Nations and Inuit communities, and increase the amount of Indigenous workers in the healthcare field at large."
The initiative has two Activities which are 1) Post-secondary bursaries/scholarships; and, 2) Community-based training.
Each Activity flows into a respective Output. Activity 1) Post-secondary bursaries/scholarships flows into, and is noted as having a "Direct Influence" on the achievement of, the Output of "Bursaries and scholarships for indigenous students in health programs. Activity 2) Community-based training flows into, and is noted as having a "Direct Influence" on the achievement of, the Output of "Training for Community-based workers (including Health Managers)."
Both Outputs flow into, and are noted as having a "Direct Influence" the achievement of, the Immediate Outcomes of "Indigenous people participate in post-secondary education leading to health careers" and "Community-based workers are trained to improve the quality and consistency of healthcare services in First Nation and Inuit communities".
The Immediate Outcomes flow into, and are noted as having a "Contributing Influence" on the achievement of, the Intermediate Outcomes of "Greater capacity of health and/or community workers in First Nation and Inuit communities" and "Indigenous people are working in the health sector."
The Intermediate Outcomes flow into, and are noted as having a "Contributing Influence on the achievement of, the Ultimate Outcomes of "First Nations and Inuit are able to influence and/or control (design, deliver, and manage) health programs and services.
And finally the Ultimate Outcomes flow into the Strategic Outcome (Program Alignment Architecture) of "First Nation and Inuit communities, families, and individuals receive health services and benefits that are responsive to their needs so as to improve their health status."